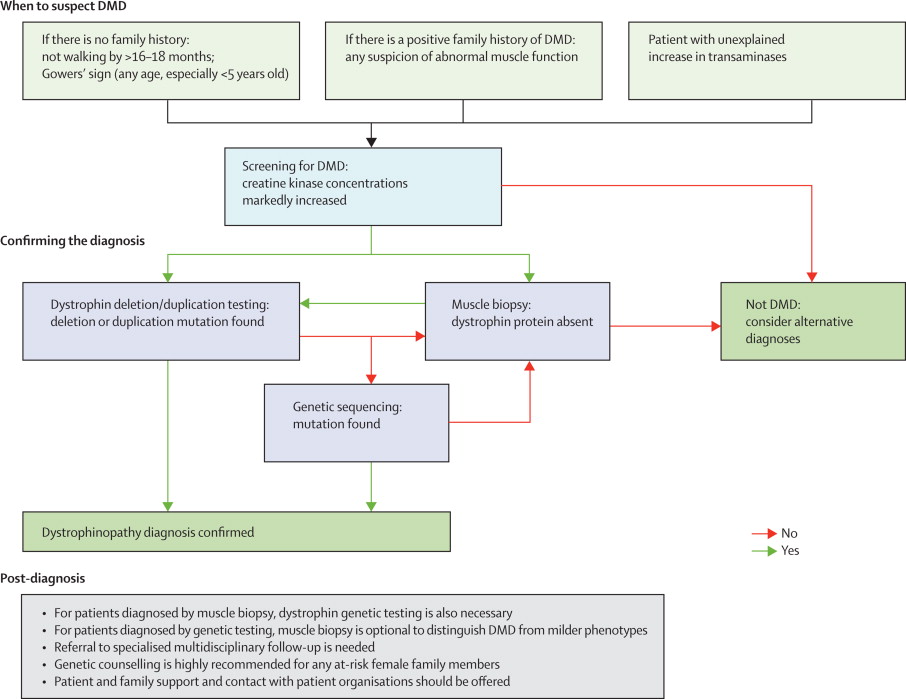
Problems with the protein Dys manifest themselves in persons as DMD. This disease affects only males and is inherited in the female line. Symptoms are apparent around the ages of two to five as walking deficiencies are commonly present once the child begins to ambulate. The major characteristic of the disease is the muscular wasting and weakness with concurrent hypertrophy of other muscles. Other clinical features include creatine kinase (CK) enzyme levels to be markedly elevated in males with DMD. An elevation in CK (a marker for muscle damage) of 30 to 300 times the normal level of < 250 U/l is common in persons with DMD. When diagnosing DMD, a neuromuscular specialist should first consider the presence of abnormal muscle function, elevation in CK, and the discovery of transaminases, before a biopsy is performed. There is no cure for DMD, but recent advances in therapy have been able to prolong the lifespans of persons with DMD (a detailed outline of DMD diagnosis is presented in Figure #1).
All striated muscle (heart and skeletal) appears to be affected by the dystrophin deficiency. Muscle weakness increases at a slow pace, and contractures of the hips and ankles develop before the age of 10. Usually between the ages of eight and 12 years severe contractures and muscle weakness are apparent, and most children are unable to ambulate. Loss of ambulation may lead to secondary conditions such as pressure sores and obesity. Additionally, the respiratory muscles are also affected which leads to frequent respiratory infections and eventual death due to respiratory failure between the ages of 15 and 25. The smooth muscle controlling bowel and bladder remain unaffected in persons with DMD, thus sparing these persons additional problems with these systems.
Figure 1: